CONNECT ACT Fact Sheet
The Center for Connected Health Policy released a fact sheet on the Creating Opportunities Now for Necessary and Effective Care Technologies (CONNECT) for Health Act of 2021.
Dr. Raed Azzam, an epileptologist with the Cleveland Clinic Neurological Institute, talks with a patient during a telemedicine appointment at his office at the Cleveland Clinic Akron General Wellness Center in March. While telehealth appointments aren’t new, they’re being used with greater frequency because of the COVID-19 pandemic, especially for mental health services, and are likely here to stay.
After a year of talking with patients via Zoom, phone and sometimes FaceTime, some mental health providers are confident that telemedicine is here to stay, even after the pandemic goes away.
Kristen Carpenter, director of ambulatory services at Ohio State Harding Hospital, said the hospital did some telehealth services before the pandemic, but it mostly was used to connect different emergency rooms and to provide emergency psychiatric care. But with COVID-19, the hospital went from providing “almost 100 percent in-person care to almost 100 percent care via telehealth” almost immediately, she said.
Now, with about 90 percent of Harding’s outpatient care still provided via telehealth, Carpenter said she foresees a future where patients can choose how they’d like to receive their care.
“Our patients have experienced almost no interruption in their care,” she said. “We have been able to provide care that we never thought we could do via telehealth.”
Harding currently offers individual counseling and psychiatry services in person and via telehealth. Its partial hospitalization and intensive outpatient program — a structured three- to four-week treatment program that typically requires patients to attend full-day group sessions in the hospital — now takes place over Zoom.
John Dawson, interim president and CEO of Community for New Direction in Columbus, Ohio, also sees telemedicine in the nonprofit group’s future — even though it had offered no telehealth services before the pandemic.
“We have a higher show rate. There’s so many barriers to mental health and substance use disorder patients getting to appointments that telehealth has helped tremendously in that area,” he said.
A new study finds during the first few months of the pandemic, patients were more likely to use telehealth services for behavioral health treatment than physical conditions, according to a January study published recently by RAND Corp. The study shows that 53.6 percent of patients with a behavioral health condition sought treatment via telehealth from mid-March to early May of 2020. By comparison, 43.2 percent of patients with a chronic physical condition used telehealth to receive care during the same period.
Providing services via phone or video conferencing has broken down many barriers including unreliable access to transportation and work conflicts, Carpenter said. At Harding, for example, there are fewer emergency cancellations and lower no-show rates because of telehealth appointments, she said.
As with other things provided remotely, however, there are some drawbacks.
Linda Jakes, executive director of Concord Counseling Services in Westerville, Ohio, said the nonprofit group found it a bit more difficult in particular o treat young children and older adults remotely. Both groups tend to be more difficult to engage, she said, and older adults sometimes have more trouble navigating technology than other patients.
“It could be difficult when you’re just having a phone conversation with someone to really see the body language associated,” Jakes said. “There’s a lot of things that we use our eyes for.”
There are other challenges as well, said Dawson of Community for New Direction.
Having reliable internet and access to a private space for appointments are privileges that some people simply don’t have, he said.
To address telehealth accessibility, he said his agency is working to provide funding for data cards and phones for patients in need.
Aside from accessibility, some patients must be seen in person, Dawson said. Those include individuals with severe opiate use disorder or personality disorders, for instance, who require closer assessment. All patients, he added, come into the office for their intake paperwork and subsequent drug tests, if it is part of their treatment plan.
Concord Counseling has established safety protocols such as staggered appointment times and alternating days that employees come in, but otherwise is letting individual clinicians decide when they want to bring patients into the office, said Mike Preston, director of clinical operation. He said most providers have in-person appointments with patients for whom “telehealth is just not working for them.”
Carpenter said having mostly virtual appointments has been draining for providers, who sit in front of computer screens for hours at a time without breaks. And though mental health treatment lends itself to telehealth, the social interaction that in-person care provides is lost in virtual appointments.
“As the year has progressed, we’ve focused a lot on how coming into the office can actually be a kind of intervention for behavioral health, to draw them back out into the world,” she said.
Jakes said telehealth has been invaluable and she can’t imagine returning to offering only in-person care. But she said many clinicians are looking forward to certain milestones that they didn’t appreciate before the pandemic.
“I was talking to one of our therapists the other day and she goes, ‘Oh my God, it’s going to be so exciting to come back,’ because she has a chunk of her caseload that she’s never even met, she’s only done telehealth,” Jakes said. “She goes, ‘If I passed them on the street, I wouldn’t even know who they are.’”
We are excited to announce that there will be a conversation on efforts to expand rural broadband access across South Carolina, featuring State Senator Thomas Alexander, and panelists from Palmetto Care Connections, Charter Communications, and Connect The Future. On May 24 at 1:00 pm
We are very pleased to announce that Charter Communications will also present a digital device grant of 25 Chromebooks to Palmetto Care Connections, ultimately supporting digital literacy training and telehealth access points. Charter Communications is proud to offer the devices as a part of the company’s ongoing efforts to close the digital divide and to support Palmetto Care Connection’s work to bring telehealth to South Carolinians.
Posted May 13, 2021
COLUMBIA, S.C. South Carolina’s state government will get almost $2.5 billion in new COVID-19 relief, with millions more headed to the state’s counties and cities tied up in the administration’s latest $350 billion round of federal coronavirus aid announced this week.Every one of the state’s 46 counties and a handful of cities will get a share of the relief.
Lexington County will get $58 million, and Richland County will take $80 million. Charleston County will take home almost $80 million, and Greenville County, one of the state’s fastest-growing counties, will get more than $101 million. Horry County is slated to get $68 million, and $54 million will go to York County.
Out of about $66 million total, the city of Columbia will get more than $27 million, the city of Charleston will get $21 million and Greenville will get $17.9 million. Among the coastal cities, the federal government will send $5.2 million to Hilton Head Island, almost $8 million to Myrtle Beach and almost $2 million to North Myrtle Beach. Rock Hill in York County will get $13 million.
The Biden administration announced the new aid Monday, part of the president’s $1.9 trillion coronavirus package signed into law in March.
The White House said payouts could be coming to state and local governments in the coming days.
For local governments, money is slated to come in two rounds with half paid out this month and the remaining a year from now. Meanwhile, states that recorded a 2-percentage-point hike in unemployment rates relative to February 2020 will get their checks in a single payment. The rest will get their money in two rounds.
The state, counties and cities will have broad powers over how they can spend the money from the U.S. Treasury, officials said.
Uses of the money could include mitigating public health costs, addressing COVID-19 financial hardships that families face, helping small businesses, revitalizing tourism and hospitality, investing in expanding broadband internet and fixing sewer and water infrastructure.
And states could use the money to defray costs for vaccinations, COVID-19 testing, contact tracing and personal protective equipment.
Governments cannot use the federal aid to cover any tax cuts, pay down debts or enhance emergency reserve accounts.
The Legislature spent $208 million earlier this year to cover vaccination efforts and coronavirus testing. In that legislation, lawmakers included a measure that would allow the state to use federal dollars before state money to pay for those efforts.
“We all know that one of the things that held back the recovery the most after the Great Recession was the contraction of state and local government,” said Gene Sperling, the administration official overseeing aid distribution for the White House, the Associated Press reported. “This is responding to the lessons of the past in a powerful way.”
The news follows Gov. Henry McMaster’s announcement last week that the state would pull out of the federal government’s pandemic unemployment program, providing an extra benefit to unemployed people.
Starting June 30, the state will no longer be part of the program through the state Department of Employment and Workforce.
South Carolina’s economy has rebounded better than many other states, avoiding budget cuts that other states reported, though its unemployment rate slipped down to 5.1% in March from 5.2% in February.
But the state, McMaster said, has another problem: the state has more than 81,000 available job openings, and McMaster and other leaders say the added now $300-a-week unemployment bump is encouraging people to stay out of the workforce.
Democrats, workers’ advocates and civil rights leaders have rejected that argument and condemned the governor’s order, saying that many have stayed out of the workforce for a whole host of reasons that may include lack of access to childcare.
“What was intended to be a short-term financial assistance for the vulnerable and displaced,” during the COVID-19 pandemic, McMaster wrote last week to jobs director Dan Ellzey, has “turned into a dangerous federal entitlement, incentivizing and paying workers to stay at home rather than encouraging them to return to the workplace.
Read more here: https://www.thestate.com/news/coronavirus/article251317163.html#storylink=cpy
May 12, 2021
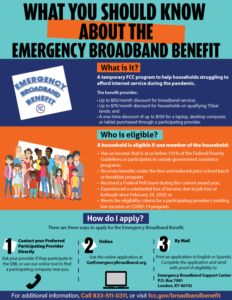
The Federal Communications Commission has launched a temporary program to help families and households struggling to afford Internet service during the COVID-19 pandemic. The Emergency Broadband Benefit provides a discount of up to $50 per month toward broadband service for eligible households and up to $75 per month for households on qualifying Tribal lands. Eligible households can also receive a one-time discount of up to $100 to purchase a laptop, desktop computer, or tablet from participating providers.
Eligible households can enroll through a participating broadband provider or directly with the Universal Service Administrative Company (USAC) using an online or mail in application.
You can learn more about the benefit, including eligibility and enrollment information, by visiting www.fcc.gov/broadbandbenefit, or by calling 833-511-0311
Posted May 6, 2021
With lessons learned from the coronavirus pandemic, health systems and telehealth vendors are shaping their connected health strategies – and identifying key trends – for years to come.
The $3.2B Emergency Broadband Benefit program provides a discount of up to a $50 per month toward broadband service for eligible households and up to $75 per month for qualifying households on qualifying Tribal lands. The benefit also provides up to a $100 per household discount toward a one-time purchase of a computer, laptop, or tablet if the household contributes more than $10 and less than $50 toward the purchase through a participating broadband provider.
A household is eligible if one member of the household meets at least one of the criteria below:
Emergency Broadband Benefit enrollment will begin (opened) on May 12, 2021. Eligible households can enroll through a participating broadband provider or directly with the Universal Service Administrative Company (USAC) using an online or mail-in application. Additional information about the Emergency Broadband Benefit is available at www.fcc.gov/broadbandbenefit, or by calling 833-511-0311 between 9 a.m. and 9 p.m. any day of the week.
Click Here to view image.
FCC NOW ACCEPTING APPLICATIONS FOR ROUND 2 OF
COVID-19 TELEHEALTH PROGRAM
Application Window Open April 29-May 6, Will Provide an Additional $249.95 Million to Support Health Care Providers and Patients In All 50 States, DC, and Territories
WASHINGTON, April 29, 2021—The Federal Communications Commission today announced the application window for Round 2 of the COVID-19 Telehealth Program is now open. Applications will be accepted through Thursday, May 6, 2021 at 12:00 PM ET. Round 2 of the COVID-19 Telehealth Program is a $249.95 million federal initiative that builds on the $200 million program established as part of the CARES Act. Applications can be submitted online at https://www.usac.org/about/covid-19-telehealth-program/.
“I’m pleased to announce that eligible health care providers can now apply for the second half of funding for the FCC’s COVID-19 Telehealth Program,” said Acting Chairwoman Jessica Rosenworcel. “This program has helped provide a lifeline to health care providers by expanding connected health services during the pandemic. I’d like to extend my continued gratitude to our FCC team for quickly standing up the second phase of this important program.”
The FCC’s COVID-19 Telehealth Program supports the efforts of health care providers to continue serving their patients by providing reimbursement for telecommunications services, information services, and connected devices necessary to enable telehealth during the COVID-19 pandemic.
For additional information on eligibility and the application process, review the Application Process Guidance available on the Universal Service Administrative Company’s COVID-19 Telehealth Program webpage at https://www.usac.org/about/covid-19-telehealth-program/. Questions specific to the application process should be directed to [email protected].
###Media Relations: (202) 418-0500 / ASL: (844) 432-2275 / Twitter: @FCC / www.fcc.gov
This is an unofficial announcement of Commission action. Release of the full text of a Commission order constitutes official action. See MCI v. FCC, 515 F.2d 385 (D.C. Cir. 1974).
For Immediate Release
April 29, 2021
Contact:
Mike Inacay (202) 224-3123
SCHATZ, WICKER LEAD BIPARTISAN GROUP OF 50 SENATORS IN REINTRODUCING LEGISLATION TO EXPAND TELEHEALTH ACCESS, MAKE PERMANENT TELEHEALTH FLEXIBILITIES AVAILABLE DURING COVID-19 PANDEMIC
Telehealth Use Among Medicare Beneficiaries Increased By 13,000% In Just A Month And A Half During The Pandemic
CONNECT For Health Act Holds Broad Bipartisan Support, Most Comprehensive Legislation On Telehealth In Congress
WASHINGTON – Today, U.S. Senators Brian Schatz (D-Hawai‘i), Roger Wicker (R-Miss.), Ben Cardin (D-Md.), John Thune (R-S.D.), Mark Warner (D-Va.) and Cindy Hyde-Smith (R-Miss.) led a bipartisan group of 50 senators in reintroducing the Creating Opportunities Now for Necessary and Effective Care Technologies (CONNECT) for Health Act of 2021. The CONNECT for Health Act will expand coverage of telehealth services through Medicare, make permanent COVID-19 telehealth flexibilities, improve health outcomes, and make it easier for patients to safely connect with their doctors.
“The last year has shown us that telehealth works, it’s popular, and it’s here to stay,” said Senator Schatz. “Our comprehensive bill makes it easier for more people to safely get the care they need no matter where they live.”
“Telehealth is enabling more people to receive the care they need, leading to improved outcomes and lower costs,” Senator Wicker said. “This bipartisan legislation would build on the success of telehealth in states like Mississippi to eliminate existing barriers and expand access to lifesaving care for more Americans.”
Three provisions from the CONNECT for Health Act were included in COVID-19 relief legislation to expand access to telehealth during the pandemic. As a result, telehealth has seen a sharp rise in use since the start of pandemic as patients seek to avoid traveling to hospitals and other health care settings and instead receive care at home. Data shows that the number of Medicare beneficiaries using telehealth services increased by about 13,000 percent in just a month and a half during the pandemic.
“The COVID-19 pandemic has demonstrated telehealth’s utility in delivering essential care. As we look beyond the pandemic, it is clear that telehealth will be a crucial tool in addressing health disparities for populations with diminished access to care,” said Senator Cardin. “I’m proud to continue partnering with my colleagues on this bipartisan bill that will increase the availability of telehealth and help deliver better health care to Americans in every part of Maryland and across the country.”
“South Dakotans were utilizing telehealth services long before the pandemic, and they understand the value and increased access it brings,” said Senator Thune. “We’ve learned plenty from the pandemic, and it’s now all the more clear how important it is to continue to expand access to telehealth. I appreciate the opportunity to work with my colleagues and stakeholders on this important bill that will make it easier for patients to use telehealth.”
“If we’ve learned anything in the past 14 months, it’s that people are better off when they’re able to see a doctor quickly, easily, and from the comfort of home. This is particularly the case for folks in rural or medically underserved communities, who may otherwise have to travel long distances to get basic medical services,” said Senator Warner. “I’m proud to introduce this legislation, which will enable Virginians to make the most of telehealth capabilities and access the quality and affordable health care they need as soon as they need it.”
“The past year has highlighted the value of telehealth, and those benefits will increase with rapidly advancing technology,” said Senator Hyde-Smith. “This legislation would help ensure Mississippians and Americans can continue to rely on telehealth services for easier access to affordable, quality care, even after the pandemic ends.”
In addition to Senators Schatz, Wicker, Cardin, Thune, Warner, and Hyde-Smith, the CONNECT for Health is cosponsored by U.S. Senators Jon Tester (D-Mont.), Rob Portman (R-Ohio), Martin Heinrich (D-N.M.), Lisa Murkowski (R-Alaska), Sheldon Whitehouse (D-R.I.), Steve Daines (R-Mont.), Chris Murphy (D-Conn.), Tim Scott (R-S.C.), Angus King (I-Maine), Thom Tillis (R-N.C.), Tom Carper (D-Del.), Kevin Cramer (R-N.D.), Tina Smith (D-Minn.), Ben Sasse (R-Neb.), Chris Van Hollen (D-Md.), Susan Collins (R-Maine), Maggie Hassan (D-N.H.), John Barrasso (R-Wyo.), Jeanne Shaheen (D-N.H.), John Boozman (R-Ark.), Amy Klobuchar (D-Minn.), Shelley Moore Capito (R-W.Va.), Richard Blumenthal (D-Conn.), Jim Inhofe (R-Okla.), Tim Kaine (D-Va.), Tom Cotton (R-Ark.), Patrick Leahy (D-Vt.), Joni Ernst (R-Iowa), Krysten Sinema (D-Ariz.), Jerry Moran (R-Kan.), Bernie Sanders (I-Vt.), Dan Sullivan (R-Alaska), Chris Coons (D-Del.), John Hoeven (R-N.D.), Raphael Warnock (D-Ga.), Roy Blunt (R-Mo.), Michael Bennet (D-Colo.), Marco Rubio (R-Fla.), Mark Kelly (D-Ariz.), James Lankford (R-Okla.), Cory Booker (D-N.J.), Lindsey Graham (R-S.C.), Jacky Rosen (D-Nev.), and Bill Cassidy (R-La.).
The CONNECT for Health Act was first introduced in 2016 and is considered the most comprehensive legislation on telehealth in Congress. Since 2016, several provisions of the bill were enacted into law or adopted by the Centers for Medicare & Medicaid Services, including provisions to remove restrictions on telehealth services for mental health, stroke care, and home dialysis.
The updated version of the CONNECT for Health Act builds on that progress and includes new and revised provisions that will help more people access telehealth services. Specifically, the legislation will:
Companion legislation has been introduced in the House of Representatives by U.S. Representatives Mike Thompson (D-Calif.), Peter Welch (D-Vt.), David Schweikert (R-Ariz.), Bill Johnson (R-Ohio), and Doris Matsui (D-Calif.).
The CONNECT for Health Act has the support of more than 150 organizations including AARP, America’s Essential Hospitals, American College of Emergency Physicians, American Hospital Association, American Heart Association, American Medical Association, American Medical Group Association, American Nurses Association, American Telemedicine Association, Children’s National Hospital, eHealth Initiative, Federation of American Hospitals, Health Innovation Alliance, HIMSS, National Alliance on Mental Illness, National Association of Community Health Centers, National Association of Rural Health Clinics, National Rural Health Association, Personal Connected Health Alliance, and Teladoc Health.
“Our thanks go to longstanding telehealth champions Sen. Schatz, Sen. Wicker, and the 50 co-sponsors of this bipartisan bill, for their continued efforts to make access to telehealth a permanent part of care delivery in our country,”
said Ann Mond Johnson, CEO of the American Telemedicine Association (ATA). “By ensuring Medicare beneficiaries do not lose access to telehealth after the COVID-19 Public Health Emergency ends, the CONNECT ACT protects seniors from the telehealth cliff. The ATA remains committed to working with Congress to advance swift, comprehensive policy that will explicitly ensure that everyone has access to safe, effective, and appropriate care when and where they need it, no matter where they live.”
“Federal action to expand telehealth services during the pandemic has been a lifeline that helped keep patients connected to care and allowed health centers to keep their doors open,” said Tom Van Coverden, president and CEO of the National Association of Community Health Centers (NACHC). “For patients on Medicare, especially people living in rural areas, without access to smart phones or reliable broadband, expanded telehealth flexibilities are essential to health and wellness. We cannot reverse progress, especially now. The CONNECT for Health Act ensures health centers can permanently extend these services for our Medicare population and the underserved. We are deeply grateful for the leadership of Senators Brian Schatz and Roger Wicker, as well as their colleagues on the Senate telehealth working group, in advancing this important legislation.”
A summary of the bill and the full list of endorsing organizations are available here.
April 27, 2021
On April 15, the Federal Communications Commission (FCC) announced that the application window for the Round 2 of the COVID-19 Telehealth Program will open on April 29 and close on May 6. Previously, on March 30, the FCC released a Report and Order detailing the application process for its COVID-19 Telehealth Program’s second round of funding (Round 2). Health care providers (HCPs) must have an approved eligibility determination from USAC to receive Round 2 funding.
To stay informed about Round 2 of the FCC’s COVID-19 Telehealth Program, visit USAC’s website and sign up for COVID-19 Telehealth email outreach.
The application filing window will open on Thursday, April 29, 2021 at 12:00 p.m. ET, and will close on Thursday, May 6, 2021 at 12:00 p.m. ET. USAC is hosting a series of trainings, including a Tribal training, in the lead up to the window opening to help HCPs prepare to apply. Register below to join these trainings and visit the COVID-19 Telehealth resources page to watch the training recordings after the training date has passed:
COVID-19 Telehealth Overview on April 22 at 1 p.m. ET: Watch Recording
COVID-19 Telehealth Eligibility on April 26 at 2 p.m. ET: Watch Recording
COVID-19 Telehealth Program Training for Prospective Tribal Applicants on April 26 at 4:30 p.m. ET: Watch Recording
COVID-19 Telehealth Application Process on April 28 at 1 p.m. ET: Register
In the meantime, HCPs can prepare for the application filing window by confirming that they have an approved eligibility determination with USAC, signing up for an FCC Registration Number (FRN) through the Commission Registration System (CORES), if they haven’t already done so, and completing their federal System of Award Management (SAM) registration, if necessary.
Palmetto Care Connections (PCC) is the telehealth network for South Carolina that offers telehealth support services to rural and underserved health care providers.
![]()
© 2026 Palmetto Care Connections. LLC
Site by Catoe Group · Inspiring digital commerce.™