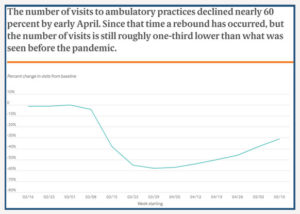
Since March, researchers at Harvard University and Phreesia, a health care technology company, have been tracking and analyzing data on changes in visit volume and use of telemedicine for 50,000 providers who are Phreesia clients. Visits were captured from February 1 through June 20, 2020. A visit was counted if it was in the practice’s scheduling software and the patient was “checked in.” The data excludes any new Phreesia clients who joined after February 15th, 2020.
In late June, the researchers released the third update to their findings, reflecting trend data since March. Key findings from their previous two reports included that there was a 60% decline in ambulatory care visits when the pandemic began, which continued into the end of April. In mid-May, data suggested that a rebound was beginning. Researchers note in this latest report that while visit numbers have rebounded, they are still substantially lower than before the pandemic.
For telemedicine visits specifically, researchers were able to identify those based on notes regarding appointment type or location made in the scheduling software. Telemedicine included both telephone and video visits in this study. Not surprisingly, starting in March, as in-person visits dropped, telemedicine visits increased rapidly. Since a peak in mid-April, telemedicine use has begun to decline, though levels remain higher than prior to the pandemic. Telehealth utilization data tracking numbers from Fair Health also show similar spikes in utilization in April.
The researchers acknowledge some of the study limitations, including that some visits may not have been captured in the software, especially unscheduled telephone encounters. Additionally, early in the pandemic, processes were still being created to designate telemedicine visits within the scheduling software, which may mean that some of that data was not initially captured. See the full study findings for more detailed information.
A new telehealth bill in the US House of Representatives released late last week aims to make some of the telehealth expansions in Medicare that require a change in law permanent. The bill would allow the Secretary to waive or modify any requirements associated with telehealth services during an emergency, disaster or a public health emergency and ending 90 days after its expiration. It would also eliminate the requirement that the patient be located in a rural area in order to be eligible for reimbursement under Medicare as well as allow the patient to be located in their home, starting January 1, 2021. FQHCs and RHCs would be added as eligible telehealth distant site providers. Finally, the new House bill would require the Secretary of Health and Human Services, acting through the CMS Administrator to submit a report to congress on telehealth service utilization as well as assessment of benefits and barriers experienced during the emergency period. This bill coincides with the publication of CMS Administrator Seema Verma’s latest Health Affairs Blog, which indicates that at least some of the administrative changes CMS has made to expand telehealth reimbursement could be made permanent. The blog indicates that as part of the CMS review, they are looking at “the impact these changes have had on access to care, health outcomes, Medicare spending and impact on the health care delivery system.” Stay tuned for future updates from CCHP.
A Bamberg-based telehealth network has received a federal grant to establish a virtual access telehealth network and expand access to health care delivery to select cities and towns in The T&D Region.
Palmetto Care Connections received a $300,000 Rural Health Network Development grant for each of three years to expand health care delivery of the rural underserved population in Orangeburg, North, Neeses, Cope, Ehrhardt, Murrells Inlet and St. George.
The U.S. Department of Health and Human Services’ Health Resources and Services Administration awarded the grant.“The COVID-19 pandemic has certainly changed the way that health care is being delivered, and this grant will help us build on the progress that has been in made and implement telehealth in some innovative ways at rural pharmacies, churches and a tribal community resource center,” CEO Kathy Schwarting said.
Under the grant, PCC will expand its existing rural health network to establish the South Carolina Virtual Access Telehealth Network (SC VATN) by adding rural, independent pharmacies, Medical Ministries Inc., Pine Hill Indian Community Development Initiative and health care providers to the telehealth network services.
The purpose of the project is to expand access to care in the target communities by integrating the functions of network members, staff, and the board of directors to improve population health as well as individual health outcomes.
Network project activities will include: implementing telehealth services; specialty and primary care integration; improving coordination of services; implementing health information technology/exchange; and implementing programs to increase primary care workforce in rural communities.
Expected program outcomes include an improvement in quality of life among chronic disease patients, an improvement in blood pressure control among hypertension patients, an improvement in HbA1c in diabetes patients, and an improvement in knowledge and/or skills among pharmacists and providers.
The SC VATN will consist of 15 members.
Four of the members are rural, independent pharmacies: Ehrhardt Pharmacy in Ehrhardt; Giant Discount Pharmacy in Neeses, R&J Drugs in North; and Lee’s Inlet Apothecare in Murrells Inlet.
One is a non-profit organization, Medical Ministries, Inc., that operates clinics in three rural churches — Good Hope AME Church in Cope, Edisto Fork United Methodist Church in Orangeburg, and Bethel AME Church in St. George.
One is a tribal affiliated community organization, Pine Hill Indian Community Development Initiative.
Other members include Family Health Centers Inc.; CareSouth Carolina; Bamberg Family Practice; MUSC; USC School of Medicine; BlueCross BlueShield of SC; PRISMA Health; South Carolina Hospital Association and South Carolina Office of Rural Health.
Established in 2010, PCC is a nonprofit organization that provides technology, broadband, and telehealth support services to health care providers in rural and underserved areas in the state.
In a commentary in Health Affairs, CMS Administrator Seema Verma laid out the numbers for telehealth use by Medicare beneficiaries from March through June, and said the agency is still working on a plan for long-term coverage.
– More than 9 million Medicare beneficiaries used telehealth during the early stages of the coronavirus pandemic, according to data from the Centers for Medicare & Medicaid Services, with a weekly jump in virtual visits from 13,000 pre-pandemic to almost 1.7 million in April.
The information, contained in a July 15 Health Affairs commentary penned by CMS Administrator Seema Verma, points to the rapid uptake of connected health use from March 17 through June 30, spurred by the crisis and state and federal efforts to relax telehealth rules to encourage adoption. It also comes as healthcare providers await information from CMS as to how these temporary measures might be made permanent.
“Telehealth will never replace the gold-standard, in-person care, (but it does serve) as an additional access point for patients, providing convenient care from their doctor and health care team and leveraging innovative technologies that could improve health outcomes and reduce overall health care spending,” Verma said. “The rapid explosion in the number of telehealth visits has transformed the health care delivery system, raising the question of whether returning to the status quo turns back the clock on innovation.”
“The data have shown that telehealth can be an important source of care across the country, not just for those living in rural areas,” she added. “Additionally, the immediate uptake in telehealth demonstrates the agility of the health care system to quickly scale up telehealth services, so that health care providers can safely take care of their patients while avoiding unnecessary exposure to the virus.”
According to that data, compiled from Medicare FFS claims:
Some 22 percent of telehealth beneficiaries in rural areas used telehealth during that time frame, while 30 percent of urban beneficiaries sought virtual care;
More than 35 percent of beneficiaries in the Northeast – specifically, Massachusetts, Rhode Island, Connecticut, New Jersey, Delaware and Maryland – used telehealth, compared to less than 17 percent telehealth use among beneficiaries in Nebraska, Montana, Idaho and the Dakotas;
One-quarter of all male beneficiaries accessed telehealth during the time period, while 30 percent of female beneficiaries used it;
Some 34 percent of people between below age 65 used telehealth, a higher rate than those between the ages of 65 and 74 (25 percent) and 75 and 84 (29 percent), as well as those over 85 (28 percent);
Some 28 percent of people identifying themselves as white access telehealth, while 25 percent of Asians, 29 percent of Blacks, 27 percent of Hispanics and 26 percent of those identifying as “other” used connected health;
Roughly 34 percent of dual-eligible beneficiaries used telehealth, compared to 26 percent of those only on Medicare, with use spread evenly over racial and ethnic groups;
The most common form of connected health visit was the evaluation and management (E/M) visit, used by nearly 5.8 million beneficiaries, and 38 percent of those visits conducted on a telemedicine platform;
Some 460,000 beneficiaries received telemental health care during this time;
Some 26 percent of beneficiaries received nursing home visits via telehealth;
Roughly 19 percent of the 1.5 million beneficiaries who access preventive health services during this time period used telehealth; and
More than 3 million beneficiaries access care through an audio-only phone, roughly one-third of the total number using telehealth during this time.
Looking to the future, Verma said CMS is “reviewing the temporary changes we made and assessing which of these flexibilities should be made permanent through regulatory action,” which CMS officials have said will likely be posted in the Federal Register sometime this month. To that end, the agency is focusing on three issues:
Whether the telehealth service is safe and clinically appropriate for patients – for example, whether telehealth can be used as a first point of contact between a doctor and patient, as opposed to the pre-COVID-19 standard of requiring an in-person visit first.
Whether Medicare should reimburse for telehealth services at the same rate as it does for in-person services. “Further analysis could be done to determine the level of resources involved in telehealth visits outside of a public health emergency, and to inform the extent to which payment rate adjustments might need to be made,” Verma noted. “For example, supply costs that are typically needed to enable safe in-person care (for, e.g., patient gowns, cleaning, or disinfectants) and built into the in-person payment rate are not needed in a telehealth visit. On the other hand, there are new processes that clinicians must create for telehealth visits, with associated costs.”
How these services might be used for fraudulent activities, such as practitioners who bill for more visits than they’re conducting or who are shortening their telehealth visits while still billing for the maximum payment.
“With these transformative changes unleashed over the last several months, it’s hard to imagine merely reverting to the way things were before,” Verma said. “As the country re-opens, CMS is reviewing the flexibilities the administration has introduced and their early impact on Medicare beneficiaries to inform whether these changes should be made a permanent part of the Medicare program.”
Healthcare industry groups are pushing congressional leaders to pass new legislation that will permanently expand telehealth flexibilities.
Action is needed to ensure patients and clinicians don’t fall off the “telehealth cliff” when the COVID-19 public health emergency ends, according to a letter (PDF) signed by 340 physician groups and industry associations.
If Congress does not act before the COVID-19 public health emergency expires, current flexibilities will immediately disappear, said the industry groups in a letter sent to Senate Majority Leader Mitch McConnell, R-Kentucky, House Speaker Nancy Pelosi, D-California, Senate Minority Leader Charles Schumer, D- New York, and House Minority Leader Kevin McCarthy, R-California.
Congress quickly waived statutory barriers to allow for expanded access to telehealth at the beginning of the COVID-19 pandemic, providing federal agencies with the flexibility to allow healthcare providers to deliver care virtually.
While federal agencies can address some of these policies going forward, the Centers for Medicare & Medicaid Services (CMS) does not have the authority to make changes to Medicare reimbursement policy for telehealth under the outdated Section 1834(m) of the Social Security Act, the groups said.
Organizations signing the letter include the American Academy of Family Physicians, the American Telemedicine Association, the Alliance for Connected Care, the Primary Care Collaborative, the American College of Physicians, AMGA and the College of Healthcare Information Management Executives
Technology companies also signed the letter including Epic, Cerner, Allscripts and Google.
Providers across the country have utilized recent policy flexibilities to scale delivery and provide older Americans, many for the first time, access to high-quality virtual care, resulting in 11.3 million beneficiaries accessing telehealth services in mid-April alone, according to the letter.
Additional flexibility has also allowed federally qualified health centers to deliver safe and effective care to underserved patient populations that have rated the service they received highly
Private health plans have also followed suit, and in response, telehealth adoption has soared—resulting in a 4,300% year-over-year increase in claims for March 2020, the groups said in the letter, citing data from Fair Health.
Taken as a whole, these temporary policy changes have allowed 46% of Americans to replace a canceled healthcare visit with a telehealth service during the pandemic.
“Virtual care has provided unprecedented access for patients, but it has become clear that uncertainty as to the future of telehealth under Medicare will halt or reverse further adoption and utilization—to the detriment of both patients and providers,” the groups wrote.
Congress must act to ensure that the HHS Secretary has the appropriate flexibility to assess, transition, and codify any of the recent COVID-19-related telehealth flexibilities and ensure telehealth is regulated the same as in-person services.
The healthcare groups said congressional leaders also have the responsibility to ensure that billions of dollars in COVID-19-focused investments made during the pandemic are not wasted and instead used to support the transformation of care delivery.
Here are the steps Congress should immediately take, according to the 340 groups:
Remove obsolete restrictions on the location of the patient. The industry groups would like to see Congress permanently remove the current section 1834(m) geographic and originating site restrictions to ensure that all patients can access care at home and other appropriate locations. This would allow beneficiaries across the country to receive virtual care in their homes or a location of their choosing, where clinically appropriate and with beneficiary protections and guardrails in place.
Maintain and enhance HHS authority to determine appropriate providers and services for telehealth. The HHSSecretary needs to have the flexibility to expand the list of eligible practitioners who may furnish clinically appropriate telehealth services. Similarly, HHS and CMS should maintain the authority to add or remove eligible telehealth services—as supported by data and demonstrated to be safe, effective, and clinically appropriate—through a predictable regulatory process that gives patients and providers transparency and clarity.
Ensure federally qualified health centers and ruralhealth clinics can furnish telehealth services after the public health emergency. Congress should ensure that these facilities can offer virtual services post-COVID and work with stakeholders to support fair and appropriate reimbursement for these key safety net providers
Make permanent HHS temporary waiver authority for future emergencies. The industry groups want HHS and CMS to have the authority to act quickly during future pandemics and natural disasters.
Despite reimbursement barriers, home health care providers have long used telehealth and mHealth tools to improve care. Could COVID-19 expand those opportunities?
– With the world stuck in the midst of a pandemic, health systems are looking to telehealth to shift the balance of care out of the hospital or clinic and into the home.
That strategy is shining a spotlight on the home health care industry, which has long balanced connected and in-person care but – faced with a shortage of providers and a growing surplus of patients – could use more of the former and less of the latter.
COVID-19 aside, home health care providers are looking to push the envelope on care management and coordination. They’re using telemedicine technology, ranging from mHealth apps and connected devices to remote patient monitoring and smart home programs, to provide a continuous care experience, and one that balances clinical support with self-management.
The pandemic has certainly helped that strategy, with a record number of care providers using telehealth to bypass crowded or closed hospitals and clinics and offer care at home. But while federal and state regulators have enacted a slew of emergency measures to expand telehealth access and coverage, the home health care industry has seen few benefits.
How the industry has used telehealth, and how providers are positioning themselves now to embrace more virtual services, may well sway lawmakers and policy wonks to give home healthcare providers more freedoms in the future.
How Telehealth Has Already Helped High-Risk Patients
Banner Health’s home healthcare program has been using telehealth for roughly three years, giving nurses a virtual window into the home lives of some of the Arizona health system’s most frequent healthcare users.
“It’s good to have that extra visual touch on them,” says Mandy Johnson, senior manager of Banner Home Care’s post-acute care coordination program. “And it gives us information in real time that we need” to improve care.
Johnson says Banner’s program, which partners with New Jersey-based Health recovery Solutions (HRS), gives telehealth kits with Bluetooth-enabled devices free of charge to patients who have been identified as at a high risk for hospitalization, newly diagnosed with a chronic condition or recently discharged and at a high risk of rehospitalization.
The kits allow care providers to connect virtually with patients to monitor vital signs and collect other data on a daily or weekly basis, and to see how patients go about their daily lives – a key factor in determining how to manage and adjust their care.
“They want to stay home – that’s where they’re happy,” says Johnson.
A cupboard or refrigerator filled with sugary snacks might not be the best thing for a person living with diabetes, and a few pets in the house might affect the treatment plan for someone with asthma or other breathing issues.
“The hospital is a stable environment,” Johnson says, “so we want to see the patient at home, and use that home environment to teach them” how to care for themselves and improve their health and wellness.
Patients are very receptive to the program, she says.
“They want to stay home – that’s where they’re happy.”
Johnson sees a future for more telehealth in home care, especially as mHealth sensors and connected devices become more sophisticated. Bearing in mind that the health system finances the program, she’d like to see a bring-your-own-device program put into place, giving patients the freedom to use their own devices.
“BYOD is a great option to scale” the program upwards, she says, “as long as it can be made affordable for the patient. It would help us, and you’d be using the infrastructure that the patient already has.”
Amid COVID-19, Telehealth Hits Home for Providers
At Detroit’s Henry Ford Health System, an ambitious home health care program tracks a wide range of patients, including those with chronic conditions like heart failure and COPD, cancer patients undergoing chemotherapy, those recovering from thoracic cardiovascular surgery and patients who have had heart or lung transplants.
Mary Hagen, who manages the health system’s e-Home Care program, says the program, in place for serval years, focuses on reducing the readmission rate – a troubling statistic that can cause providers to lose valuable federal funding through penalties.
The program, which sends patients home with tablets and wireless devices, enables care managers to check in with patients on a regular basis, and tracks their health through vital signs and surveys. The idea is to give providers a daily snapshot of a patient’s health, allowing them to adjust care management and spot downward trends before they become health concerns.
Hagen says the key to developing a successful program lies in not anticipating results or buy-in, but going in with an open mind.
“You can’t predict how anything will go,” she says. “You just have to try it out on every person that you can, then go from there. Once you get the (technology) in place and people start using it, you find the benefits that you never saw before.”
Hagen says providers weren’t too enthusiastic about the program at first.
“I just couldn’t figure out how they didn’t think it was cool,” she says.
Then COVID-19 hit, and “it hit home for them” – literally.
“Suddenly everyone was seeing the benefits of care at home,” she says, noting the program added another 60 telehealth kits to the 170 it had to meet demand. “This changed everybody’s thinking and allowed us to look at (home health care) differently.
As with Banner, Hagen says she’d like to see more mHealth devices introduced to the program, giving provider the ability to track more metrics at home. She’d love to track spirometry, EKG, even activity and exercise, and monitor medication adherence through connected pill bottles or other digital health tools.
“And I’d much rather the patients use their own devices,” she adds, noting the costs associated with providing telemedicine technology to the home. “There’s so much out there that we could be using” if it were supplied by patients.
She’d also like to see a home health telehealth program contained inside a health system’s electronic medical record, instead of bolted on or existing alongside the EMR. Many a program lives or dies in the ability to integrate data into a patient’s medical record, avoiding gaps in care and the challenges of accessing soiled information.
“We have a good program that’s growing like crazy,” Hagen says. “It’s really showing us the possibilities of delivering care at home. Now we need more (opportunities) to use it.”
Source: Getty Images
The Struggle to Secure Telehealth Coverage
While many home health care programs are using telehealth and mHealth tools and services in some form or another, widespread adoption has been minimal, primarily due to limited Medicare reimbursement and a reluctance from the Centers for Medicare & Medicaid Services to recognize telehealth as a legitimate service.
Home health care advocates were heartened a few years back with the development of bundled payment programs that supported telehealth services delivered in the home setting, but some of those programs have since been discontinued or modified in such a way that telehealth is restricted.
“Telehealth has actually been around for quite a while in home health – a couple of decades at least,” says William Dombi, president of the National Association for Home Care & Hospice (NAHC). “But it hasn’t worked well from a business sense.”
Medicare does allow some telehealth use in its bundled payment program for home health services as an episode of care, but those reimbursements run up against strict guidelines on who can prescribe a telehealth service and how many in-person visits are required.
With the onset of the coronavirus pandemic, federal and state regulators loosened many of the rules around telehealth access and coverage, giving providers more freedom to use different tools and platforms and expanding reimbursement opportunities.
Home health care providers, however, saw few benefits from those relaxed rules.
CMS currently does not recognize the home health care provider as a telehealth provider – instead, it allows primary care providers to prescribe telehealth services in the home, and manages the services provided by home health care companies. In other words, doctors and other practitioners can prescribe and bill for telehealth services furnished, but home health care providers can’t.
“Telehealth has actually been around for quite a while in home health – a couple of decades at least,” says Dombi. “But it hasn’t worked well from a business sense.”
In addition, telehealth visits do not count toward a home health care providers’ low-utilization payment adjustment (LUPA) threshold, which sets a minimum number of in-person visits that a care provider must complete. As Dombi notes, a provider can use connected health channels – mHealth apps and devices, telehealth visits, even phone calls – to accomplish dozens of care management goals, yet still must visit the patient to meet CMS mandates.
“We’ve got all kinds of technology in the home setting now that could be put to use,” he says, noting that a recent survey found roughly 40 percent of home health care providers are using telehealth in some form. “We fully expect that telehealth has a strong future in home health … but right now we’re just not there yet.”
But they are moving in the right direction.
As part of the federal government’s response to COVID-19, CMS is allowing home health care providers to use telehealth and mHealth tools as long as those services are part of the patient’s care plan and they don’t replace in-person visits.
“The use of technology may not substitute for an in-person home visit that is ordered on the plan of care and cannot be considered a visit for the purpose of patient eligibility or payment; however, the use of technology may result in changes to the frequencies and types of in-person visits as ordered on the plan of care,” the agency states in its notice to make that change permanent. “This rule also proposes to allow HHAs to continue to report the costs of telecommunications technology as allowable administrative costs on the home health agency cost report beyond the PHE for the COVID-19 pandemic.”
Some states are relaxing the rules around Medicaid coverage for home health care services. A new law recently enacted in Colorado, for example, allows home health care providers to prescribe and manage telehealth services.
Dombi says NAHC has had some discussions with CMS over expanding telehealth coverage and access for home health care providers, though some of those provisions would have to be handled by Congressional action.
“This is the perfect time for telehealth,” says Dombi. “We need their support.”
Ideally, he says, CMS should be integrating telehealth into the model of care for homebound patients, and it should be expanding the categories of patients who qualify for home health care, to include a wider range of people who would benefit from receiving telehealth services at home. In addition, he says, CMS should recognize home health care programs as being capable of prescribing and managing telehealth services.
Plotting a Future for Connected Care
Both federal officials and healthcare providers are anticipating that telehealth adoption will continue to increase in the wake of the COVID-19 emergency, through better federal and state regulations and an interest among providers to expand their platforms.
This includes home health programs, which will get a boost from a surge of interest in remote patient monitoring. Hospitals and health systems, eager to move more services out of the hospital, clinic or doctor’s office and into the home, will be looking to develop RPM platforms. And they’ll be looking to home care providers to facilitate those services.
“People are getting comfortable with home care, and they’re realizing they’re more than can be done at home than in the hospital,” says Johnson, at Banner Health. “Besides, every time you have to go back to the hospital, we have to start all over again. We want to get away from that as much as we can.”
Traditionally a supplementary and underutilized form of health care delivery, telehealth is now one of the frontline pillars of defense against the COVID-19 pandemic. In April 2020, a Morning Consult poll found that 23% of adults have used telemedicine services since the outbreak of COVID-19, and virtual visits surged 50% in March 2020, compared to February. By keeping patients away from busy hospitals, telehealth is helping to reduce the burden on overwhelmed care centers and the risk of infections. However, the potential applications of telehealth extend far beyond this crisis. It could help ease longstanding problems with health care costs and accessibility, particularly in underserved communities. Today, New Center policy analyst Olive Morris checks in with Mei Kwong with the Center for Connected Health Policy to explore the potential of telehealth during and after the crisis.
In a new podcast, Craig Settles explains how underserved populations can gain access to telehealth and other resources through the development of community broadband programs.
– The key to telehealth expansion in underserved communities, says Craig Settles, may very well be the development of community broadband programs.
Settles, a broadband and telehealth consultant, says both urban and rural areas struggle to access reliable broadband, the foundation on which connected health programs are built. With that access controlled in large part by corporations, it’s important to develop community partnerships that give underserved residents an opportunity to schooling, library services and healthcare.
“There are segments of the country that (broadband providers) do not consider worth their time,” he says. But a community broadband program will pool resources and create access points, and “having all those access points enables them to provide services” to people at home, or at alternative locations.
In that program, Settles is organizing partnerships between healthcare providers and barbershops or hair salons (his Cleveland sites are partnering with the Cleveland Clinic). While getting their hair done, customers are encouraged to have their blood pressure checked via an mHealth device, and are given information on high blood pressure or referred directly to a care provider based on the results.
“The barbershop represents getting people comfortable with the idea” of telehealth, he says. “People who don’t normally go see a doctor, be it because of insurance or whatever,” are intrigued by the idea of virtual care if introduced to it in a community setting.
Settles sees his pilot program in three stages. The first focuses on mHealth testing, and the second will explore how other telehealth services could be introduced in a barbershop, salon or similar community gathering.
And the third focuses on developing community broadband programs that extend high-speed access to these and other locations – locations where access is limited due to cost, excessive data caps or a lack of resources or infrastructure.
To develop these programs, he says, communities need to look at federal and state funding opportunities, such as those offered by the Federal Communications Commission, and pool together businesses, schools, libraries and healthcare providers who would benefit from reliable access to broadband services. This, in turn, would make that community more robust.
“That’s what incites people to build these broadband networks in the first place,” he says. “If I can deliver economic development by making the local healthcare system more robust, people are going to go for that.”
A bill before the Senate would extend telehealth coverage for substance abuse disorder treatment, including MAT therapy and Medicare reimbursement for audio-only phone calls, beyond the COVID-19 emergency.
– A new bill before the Senate aims to expand the telehealth platform for substance abuse treatment.
Introduced last week by Senators Rob Portman (R-OH) and Sheldon Whitehouse (D-RI), the Telehealth Response for E-prescribing Addiction Therapy Services (TREATS) Act would make permanent certain emergency actions passed during the coronavirus pandemic to boost telehealth access for substance use disorder (SUD) treatment.
While the bill’s text hasn’t yet been made public, it would reportedly include allowing care providers to skip the in-person exam requirement and prescribe controlled substances in Medicated Assistant Treatment (MAT) therapy programs via connected health. It would also expand Medicare coverage for mHealth services to include audio-only phone calls.
“The COVID-19 pandemic has affected every aspect of our lives and the increase in overdoses we’re seeing only increases the need for additional flexibility to help those suffering from addiction,” Portman said in a press release. “The roll out of telehealth waivers has both helped patients maintain access to care safely at home and increased access to care for those that didn’t otherwise have access to in-person treatment. As we move forward and look to life beyond this pandemic, we must make sure that the advances to care and access that telehealth is currently providing is not lost and that’s exactly what this bill will do.”
Mental health and substance abuse treatment providers have long lobbied the federal government to remove restrictions on virtual care for SUD treatment, clashing with those who argue that online prescribing needs to be tightly regulated. With substance abuse issues skyrocketing during the ongoing pandemic, federal officials have taken action to loosen those restrictions.
Under the Ryan Haight Online Pharmacy Consumer Protection Act of 2008, certain healthcare providers are allowed to prescribe controlled substances for treatment as long as they first conduct an in-person examination with the patient. That law offers several instances in which the in-person requirement could be waived. On March 16, the US Drug Enforcement Agency (DEA) waived that requirement by invoking the public health emergency exception caused by the COVID-19 crisis.
In addition, on March 19, the Substance Abuse and Mental Health Services Administration (SAMHSA) issued separate guidance allowing Opioid Treatment Programs and certified care providers to use prescribed drugs and conduct treatments over the phone without first meeting in person. Shortly thereafter, the DEA joined SAMHSA in issuing a letter allowing “’authorized practitioners’ to prescribe buprenorphine to new and existing OUD patients for maintenance or detoxification treatment on the basis of telehealth examination, which may include a telephone voice-only evaluation – without the need for a prior in-person exam.”
“The DEA Letter allows authorized practitioners the added flexibility of using audio-only modalities (i.e., telephone) – instead of audio-visual, real-time, two-way interactive communication system – which is required to prescribe controlled substances via telemedicine, pursuant to the aforementioned emergency exception to the federal Ryan Haight Act,” Sunny J. Levine and Emily H. Wein of the Foley & Lardner law firm wrote in a recent blog summarizing the government’s actions.
Those emergency actions will end with the public health emergency, and telehealth advocates have been working at both the state and national level to extend many of these waivers indefinitely.
Among those supporting the TREATS Act are the American Society for Addiction Medicine, American College of Medical Toxicology, Kennedy Forum, National Association of Addiction Treatment Providers, National Association of Behavioral Health, National Safety Council, Shatterproof and the Well Being Trust.
During a panel session at the American Telemedicine Association’s recent virtual conference, experts from two large health systems explained how telehealth improves care for complex patients no matter where they are.
– As healthcare providers launch telehealth programs to improve critical care management and coordination, they’re seeing value far beyond the ICU.
Indeed, as the coronavirus pandemic taxes hospital resources and a growing shortage of critical care doctors becomes more apparent, hospitals and health systems are deploying telemedicine technology to treat patients wherever they’re located.
“This is telehealth at a different level,” said Jeff Guy, MD, MSc, MMHC, FACS, vice president of Emergency and Critical Care Services with HCA Healthcare, a Nashville-based network of some 186 hospitals and more than 2,000 care locations in both the US and UK.
Guy was part of a panel session at the American Telemedicine Association’s weeklong virtual conference last week. Titled “Implementing TeleCritical Care in a Healthcare Platform,” the discussion centered on how the concept of using telehealth to improve care is evolving, to focus more on delivering quality care than where that care is delivered.
A platform that began with a focus on improving care for stroke victims is now much more complex, with networks that allow large hospitals with specialists to reach out to smaller, rural hospitals that treat critical care patients regardless of whether they have an ICU. Through this platform, the large hospital at the center of the network can manage care across the enterprise, delivering specialized care and cutting down on transfers and traffic, while the smaller hospitals can keep and care for their patients on-site.
The concept of connected critical care has led to large networks like HCA, Providence Health in the Pacific Northwest, St. Louis-based Mercy Virtual and Utah’s Intermountain Healthcare, whose medical director for critical care telehealth, William Beninati, MD, was part of the panel.
Beninati pointed out the telecritical care platforms have become a means of standardizing critical care across the health system, giving the tiny hospital in a rural community that same access to care as the big-city hospital. This gives the small hospital the tools to care for more complex patients.
That point is being proven with the COVID-19 crisis. With a telecritical care platform, the large hospital is the hub of a hub-and-spoke network, using a dedicated facility or specialized call center to manage care in the spokes. It can help to balance the patient populations at all hospitals, reducing the need for costly and potentially dangerous transfers, while also helping to cut down on ICU traffic, provider exposure to the virus and even PPE use.
Both Beninati and Guy pointed out that today’s telecritical care platforms are purposefully built to be flexible, as each hospital in the system (and those outside the system who might be able to join the platform) has different needs and capabilities. The telemedicine platform should also be easy enough that a hospital with only the most basic resources can connect.
To that end, Beninati noted that Intermountain has added an asynchronous telehealth program to its roster of services, allowing those with limited access to or need of an audio-visual platform to connect through an online portal.
This also requires the coordinating hospital to train its specialists to be adept at virtual care.
“This is a very unique skillset,” Guy said. “Because you’re a critical care physician doesn’t mean that, by default, you’re a telecritical care physician.”
Among the challenges to launching and expanding such a platform, Beninati said, is the fear among smaller providers that the telehealth platform “sucks patients out of a community.” In contrast, he said, the services does the opposite, giving those small providers the resources they need to keep patients in the community – not only for in-patient care but also for post-discharge care, including virtual visits with specialists and rehab care providers.
Other challenges include EMR integration – Beninati says Intermountain’s network has to content with several different EMR platforms – and interstate licensure and credentialing, which can be a hassle for health systems spanning several states.
The benefits, meanwhile, include reduced ER traffic at the hub hospital, a steadier care environment at the spoke hospitals, reduced transports (and the clinical and financial toll that they exact), and certain clinical benchmarks like improved sepsis detection and ventilator care, reduced length of stay and a reduced risk-adjusted mortality rate.
Palmetto Care Connections (PCC) is the telehealth network for South Carolina that offers telehealth support services to rural and underserved health care providers.